Glaucoma is one of the growing causes of vision impairment and blindness in the UK, lin 10 people aged 75 and above are affected by glaucoma, predicted to increase by 15 to 18% over 10 years.
No cure for glaucoma but we can treat.
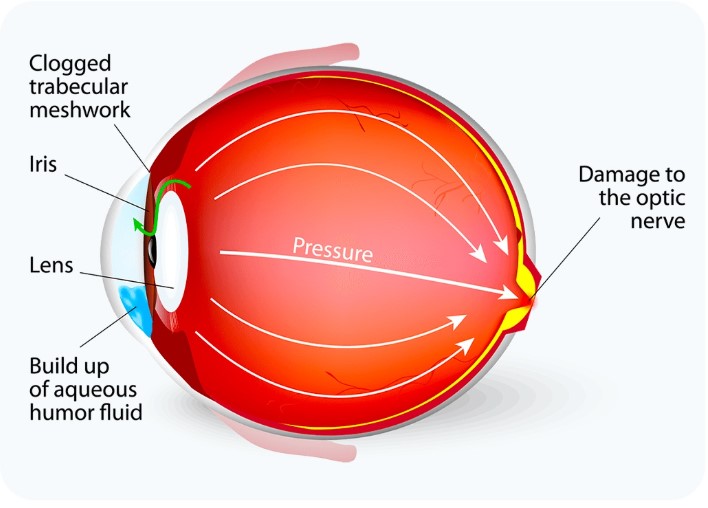
Optic nerve gets damaged due to imbalance in aqueous humour production and drainage.
Aqueous humour is a clear fluid flows through the pupil and drains through the trabecular meshwork, a spongy tissue at the drainage angle of the eye. In Glaucoma the drainage becomes inefficient or blocked (like a clogged sink), causing fluid buildup. This increases pressure inside the eye, damaging the optic nerve over time.
Is also called silent thief of sight, often no symptoms, majority of the time we don't realise that we have a problem until detected in routine testing where either eye pressure is high and or visual field changes and or optic nerve shows some damage.
Regular eye exams measuring IOP and evaluating optic nerve health and visual fields are crucial.
However, angle-closure can sometimes be silent, with no early symptoms until damage is done.
We do battery of test to prove or disprove that you have glaucoma.
We discuss all the suitable treatment options that incudes LASER'S, EYE DROPS, Operations based on the needs and patient choice.
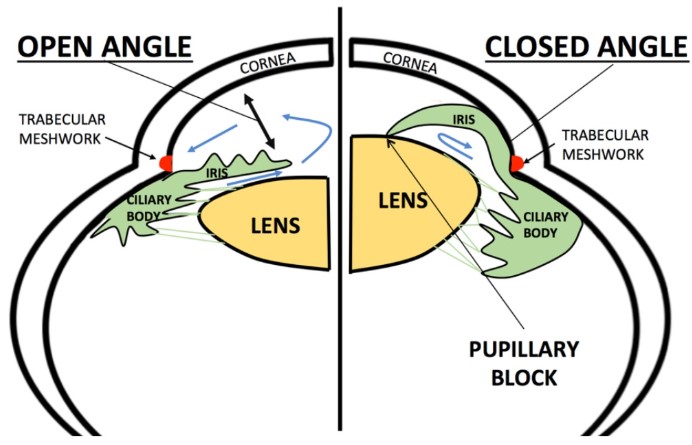
YAG peripheral iridotomy-for narrow angles with or without glaucoma.
SLT (Selective Laser Trabeculoplasty): To reduce Intraocular pressure
Cyclodiode Laser: In specific scenarios only
Glaucoma is a group of eye conditions that damage the optic nerve, usually due to elevated eye pressure. It is one of the leading causes of irreversible blindness— but when detected early, vision loss can often be slowed or prevented.
Early detection is essential because most forms of glaucoma progress silently without symptoms. A comprehensive eye exam typically includes:
Checks the pressure inside the eye. Elevated pressure can be a risk factor for glaucoma.
The eye doctor examines the optic nerve for signs of damage or structural changes.
Assesses peripheral (side) vision, which glaucoma often affects first.
Provides detailed images of the optic nerve and retinal nerve fiber layer.
Examines the drainage angle of the eye to classify glaucoma type.
Corneal thickness can influence eye pressure readings and glaucoma risk.
Glaucoma management focuses on lowering eye pressure to prevent further optic nerve damage. While vision already lost cannot be restored, treatment can preserve remaining sight.
Often the first line of treatment, They work by:
Types include prostaglandin analogs, beta-blockers, alpha agonists, and carbonic anhydrase inhibitors.
Sometimes prescribed when eye drops alone are not sufficient to control eye pressure.
If medications and lasers aren't effective
Follow-up appointments are crucial to check eye pressure, optic nerve health, and visual fields.
Using prescribed eye drops consistently is critical for preventing further vision loss.
See an eye care professional promptly if you experience:
(These may signal acute angle-closure glaucoma, a medical emergency.)
There are different types of glaucoma drops to control eye pressure; some are preservative-free and more eye-friendly.
Below we describe different groups of eye drops, their mechanism, and common side effects.
Prostaglandin analogues (Latanoprost, Travoprost, Tafluprost, Bimatoprost) - works by increasing uveoscleral outflow.
Common side effects: Dark eye and skin around the eye, darker and longer eyelashes, red eye, stinging.
Beta blockers = Timolol, Betaxolol (Timolol drops 0.25%, 0.5%, Timolol gel 0.5%).
Mechanism of action: Reduces aqueous humour production, can also increase outflow.
Common side effects: Dry eye, stinging, impotence, exacerbates asthma and COPD, reduced heart rate, hypotension.
Carbonic anhydrase inhibitors - (Acetazolamide tablets, Dorzolamide, Brinzolamide)
Mechanism of action: Reduce aqueous humour production.
Side effects: Stinging, red eye, metallic taste in mouth, electrolyte imbalance. Tablets are more effective but can cause kidney problems, sickle cell crisis, tingling, numbness, increased urination.
Netarsudil, Roclanda (netarsudil + latanoprost)
Mechanism: Increases uveoscleral outflow.
Common side effects: Red eye, dark eye and skin around the eye, darker and long eyelashes, stinging.
Alpha agonists(Apraclonidine 0.5%, 1%; Brimonidine 2%)
Mechanism: Reduces aqueous humour production and increases uveoscleral outflow.
Common side effects: Red eye, stinging, dry eye, itching, uveitis. Contraindicated in patients on antidepressants like amitriptyline.
Pilocarpine
Mechanism - constricts the pupil and increases outflow.
Used in emergency.
Side effects - headache, reduced night vision.
Wash your hands, shake the bottle. If possible, stand in front of a mirror, pull lower lid to create a pocket, squeeze one drop only without touching eye, and press on the corner of the eye lid at the base of the nose to prevent taste in mouth.
You may find this video on the correct way to use eye drops helpful. It is less than 2 minutes long and has captions available if needed.
Video demonstrating on how to use eye drops. Click here

Acetazolamide is a tablet that can help quickly lower pressure inside the eye. It works by reducing the amount of fluid the eye produces. Although very effective, it is usually used for short-term support rather than as an everyday, long-term treatment.
Chronic Open-Angle Glaucoma (COAG) or Ocular Hypertension (OHT)
Most people start treatment with laser or eye drops.
Acetazolamide tablets may be used when:
If your doctor suspects acute angle-closure, acetazolamide can help bring the pressure down very quickly. In these situations, a single 500 mg tablet may be given immediately (as long as it is safe for you) while urgent eye specialist care is arranged. This rapid treatment helps protect your sight.
Because acetazolamide is taken by mouth, some people can experience side effects such as tingling, tiredness, or stomach upset. For this reason, it is normally used only for short periods.
If long-term pressure control is needed, most people do better with eye-drop alternatives, such as:
These work in a similar way but tend to cause fewer whole-body side effects.
Your specialist will decide the right dose for you. Common doses range from 250 mg to 1000 mg per day, sometimes using slow-release tablets taken once or twice daily.
Acetazolamide is not suitable for everyone. It may not be used if you have:
Your doctor will check your medical history before prescribing it.
Nicotinamide is a promising research area, but it is not yet an approved glaucoma treatment. Current recommendations:
Nicotinamide tablet: A form of vitamin B3 (not niacin), being investigated for its potential to protect against vision loss in glaucoma, not by reducing eye pressure but by improving mitochondrial function and health of retinal ganglion cells (first cells to get damaged in glaucoma).
Evidence (NAMING and TAMING studies) show reduced progression by taking 1.5 g per day for 6 weeks, then twice daily for long term, but only consider if there is no liver disease. Liver monitoring is required at 2-3 months after starting and yearly thereafter. Not a substitute for standard glaucoma treatment.
Contraindicated in pregnant patients, cancer patients, or if you are on doxycycline, isoniazid, pyrazinamide, or carbamazepine.
Often advised as first line treatment for suitable patients which is effective in 7 in 10 patients up to 5 years. It can be considered or repeated any time during "management" only in suitable patients
Mechanism-Low energy cold laser targeted at pigmented trabecular meshwork, works by remodelling trabecular meshwork.
The entire appointment usually takes a few hours, though the laser treatment itself only takes about 5 to 15 minutes per eye.
Note: Seek immediate medical attention if you experience severe eye pain, sudden loss of vision, or worsening redness after the procedure.
Inflammation, mild bleeding, lens opacity, rarely double vision, eye pressure spike, slightly blurring.
Needs to sign the consent form provided you understood the risks and benefits. That, also, good opportunity to get answers for any questions related to operation. It is day care surgery, majority performed under local anaesthesia get to go home the same day of surgery with an advise to come back for follow up next day and weekly for a month based on advise on the day of surgery. Post op needs to use steroid drops for 3 months and few weeks of antibiotic drops. We may need to manipulate the glaucoma surgery to make it work optimally.
Who needs surgery: In general, if we can't prevent or reduce the progression of glaucoma damage by other means and or not suitable for other treatment options and or intolerant to drops.
One size doesn't fit all. Decision making on who and what type of surgery is crucial, which depends on patient needs and requirement, surgeon experience and expertise - best to discuss with the operating consultant.
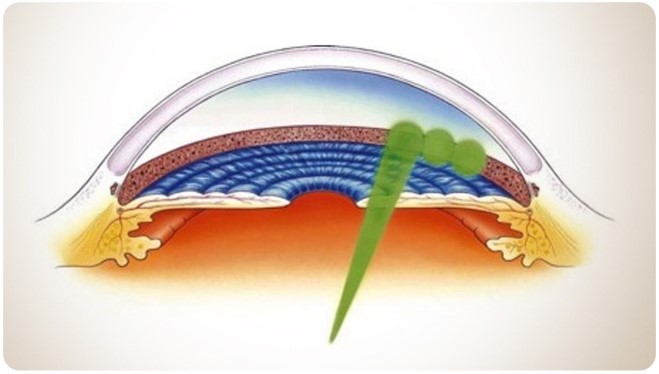
Gold standard, been performed over 50 years with success rate up to 70% over period of 5 years. Success depends on the wound healing; we use medicines to delay the healing and for better success rate. Operation involves creating a trap door on outer wall of the eye which creates a blister under eye lid to drain the fluid out of the eye.
Trabeculectomy is the most effective surgical procedure for lowering IOP, but it is also associated with a higher incidence of complications and post operative care.
Performed under local anaesthesia as a day care approximately takes an hour. Operation involves creating a trap door to drain the fluid out of the eye. Fluid collected in reservoir on outer side of the eye called “bleb” which carefully secured by releasable sutures which can be released at a later date to manipulate eye pressure to achieve “Target Eye Pressure”.
Anaesthesia: Local anaesthesia, day care operation, takes up to an hour.
Surgery: Small tube (1/3 of traditional tube) drains the fluid from anterior chamber of the eye to outer wall with success rate up to 80%.
Tube is made up inert material called SIBS, a polymer, scan and Airport friendly.
Surgery: Like above which connects to a plate on outer wall of the eye with success rate from 53 to 67%. External portion of the tube covered with patch graft secured to outer wall. These donor materials are processed and screened.
After receiving donor-derived tissue, you are no longer eligible to donate blood in the UK.
Operation is a two-stage procedure, 2nd stage may involves removing stent suture from the tube to better control eye pressure if needs adjusting.
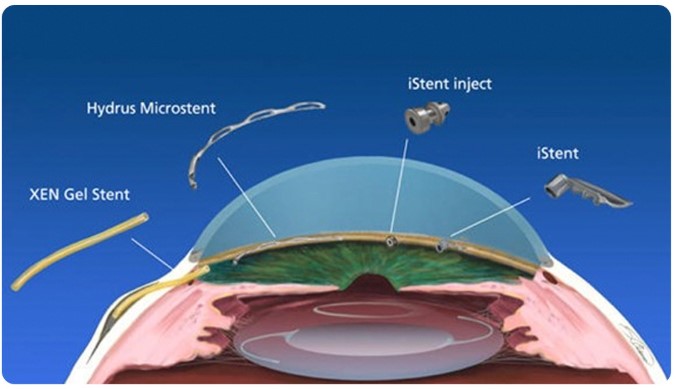
MIGS has been widely adopted by glaucoma specialists, with strong support for its benefits in treating the disease.
The decision to perform MIGS should be made by the clinician overseeing a "patient's" long-term glaucoma care.
We implant MIGS while doing cataract operation in suitable patients only.
There are several of them, some commonly used ones are KDB, I Stent, Hydrus, OMNI, MINIject, Istar.
I am a certified surgeon to perform "Hydrus Microstent, OMNI Viscodilationand visco canalostomy, MiniJet, KDB".



Cyclodiode laser photocoagulation is a glaucoma treatment that uses a diode laser to reduce the eye's production of aqueous fluid. By targeting the ciliary body (the tissue that produces fluid in the eye), the procedure helps lower intraocular pressure (IOP) in patients whose glaucoma is not controlled by eye drops, medications, or other surgeries.
This treatment is typically performed through the sclera (the white of the eye), so no incisions are required.
Cyclodiode laser is used to treat moderate to severe glaucoma, especially when:
It is effective for many types of glaucoma, including:
Patients usually go home the same day.
Most studies show:
If needed, cyclodiode laser can be safely repeated, which is helpful in difficult cases like neovascular or uveitic glaucoma.
Many patients reduce the number of glaucoma drops after treatment, though some may still require ongoing therapy.
Cyclodiode laser is generally safe, but possible risks include:
Micropulse CPC significantly reduces the risk of severe complications compared with traditional continuous-wave treatment.
Patients may continue some glaucoma medications until pressure stabilizes.
Cyclodiode laser photocoagulation is a safe, effective option for reducing eye pressure in moderate to severe or treatment-resistant glaucoma. With modern micropulse technology, outcomes have improved and complication risks have decreased, making this a valuable treatment for many patients who cannot achieve adequate pressure control with medications or traditional surgery.
